Scrotal pain sends most men straight to Google, where varicocele and epididymitis come up as the top two possibilities. They share overlapping symptoms, affect similar age groups, and both produce that nagging left-sided ache that’s hard to describe to a doctor. But the causes, treatments, and long-term implications are completely different. Misdiagnosis delays the right treatment and, in some cases, causes real harm. This guide breaks down how to tell these two conditions apart, what the diagnostic process looks like, and when each one requires urgent attention.
What Is Epididymitis?
The epididymis is a coiled tube that sits behind each testicle and transports sperm as they mature. Epididymitis is inflammation of this structure, most commonly caused by bacterial infection. In men under 35, sexually transmitted organisms like Chlamydia trachomatis and Neisseria gonorrhoeae are the primary culprits. In men over 35, urinary tract bacteria such as E. coli are more common, often associated with urinary tract infections or enlarged prostate issues.
Chronic epididymitis refers to cases lasting more than 6 weeks and often has no identifiable infectious cause. In chronic cases, inflammation, trauma, or autoimmune reactions drive persistent pain in the epididymis and surrounding scrotal tissue. This form overlaps most with varicocele in terms of symptom presentation.
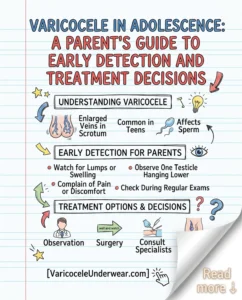
What Is Varicocele?
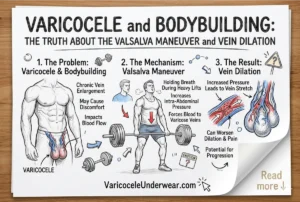
A varicocele is an abnormal dilation of the pampiniform plexus, the network of veins that drains blood from the testicle. It develops when the venous valves that prevent backflow fail, allowing blood to pool and veins to enlarge. This venous engorgement increases scrotal temperature and generates oxidative stress that damages sperm production and testicular function over time.
Varicocele is not an infection and is not contagious. It is a structural vascular problem. Understanding the full scope of varicocele as a condition helps clarify why its pain patterns and treatment approach differ fundamentally from epididymitis.
Discover specialized varicocele underwear designed for daily comfort, support, and recovery — a more targeted option for men who want support without compromise.
Discover the Recommended OptionSymptom Comparison: Varicocele vs. Epididymitis
| Symptom | Varicocele | Epididymitis |
|---|---|---|
| Pain quality | Dull, heavy ache | Sharp, throbbing, or burning |
| Onset | Gradual, over months/years | Acute (hours to days) |
| Fever | Never | Common in acute bacterial cases |
| Swelling | Veins visible/palpable | Epididymis swollen and tender |
| Urinary symptoms | Absent | Often present (burning, frequency) |
| Relief when lying down | Yes (veins decompress) | May help but not diagnostic |
| Affected structure | Pampiniform plexus veins | Epididymis (posterior testicle) |
| Bilateral occurrence | 10-15% of cases | Usually unilateral |
Key Physical Exam Differences
On physical examination, a varicocele feels like a “bag of worms” above and behind the testicle, most prominent when standing. The veins collapse when the patient lies down (in primary varicocele). The testicle itself may feel smaller than the opposite side in longstanding cases.
Epididymitis presents with a swollen, exquisitely tender epididymis, typically at the posterior-superior pole of the testicle. In severe acute cases, the entire hemiscrotum may be swollen and red (scrotal erythema), a finding never seen in uncomplicated varicocele. Prehn’s sign, where lifting the scrotum relieves pain in epididymitis but not in testicular torsion, can help but is not fully reliable for distinguishing epididymitis from varicocele in practice.
Diagnostic Tests: What Your Doctor Should Order
- Scrotal Doppler ultrasound – confirms varicocele (dilated veins, retrograde flow) and assesses epididymal size and vascularity; increased blood flow (hyperemia) on Doppler in the epididymis confirms epididymitis
- Urinalysis and urine culture – identifies bacterial infection in epididymitis; completely normal in varicocele
- STI testing – urethral swab or urine NAAT for chlamydia and gonorrhea in sexually active men under 35
- CBC and CRP – elevated white blood count and inflammatory markers in acute epididymitis; normal in varicocele
- Semen analysis – may show white blood cells (leukospermia) in epididymitis; abnormal parameters from thermal/oxidative damage in varicocele
Can You Have Both at the Same Time?
Yes, and this is more common than most patients expect. Varicocele causes venous stasis and elevated local temperature, creating a microenvironment that may predispose the epididymis to bacterial seeding and inflammation. Several case series have documented co-existing varicocele and epididymitis in the same patient, where treating only one condition left residual pain from the other.
If you’ve completed a full antibiotic course for epididymitis but still have a persistent dull ache, a scrotal Doppler ultrasound to rule out an underlying varicocele is a reasonable next step. Chronic orchialgia following treated epididymitis should not be dismissed as normal, and the pattern of your scrotal pain provides important diagnostic clues.
Treatment Differences
Acute bacterial epididymitis is treated with antibiotics, typically doxycycline plus ceftriaxone for STI-related cases, or a fluoroquinolone for urinary-source infections, for 10-14 days. Scrotal support, NSAIDs, and rest are adjunct measures. No surgery is required for uncomplicated epididymitis.

Varicocele treatment ranges from conservative management (supportive underwear, lifestyle modification) to procedural intervention (embolization or microsurgical ligation) depending on severity, symptoms, and fertility impact. Antibiotics have no role in varicocele management. For men deciding between treatment options, reviewing the varicocele treatment guide helps frame when intervention is warranted and what options exist.
For day-to-day symptom relief in either condition, cooling and supportive scrotal underwear reduces mechanical stress and venous pressure, complementing both conservative varicocele management and epididymitis recovery. Proper scrotal support is actually recommended in epididymitis treatment guidelines as standard adjunct care.
When to Go to the Emergency Room
Some scrotal conditions are emergencies. Testicular torsion (twisting of the spermatic cord) can mimic acute epididymitis and requires surgery within 6 hours to save the testicle. Never assume severe, sudden-onset scrotal pain is epididymitis or varicocele without ruling out torsion first.
- Sudden severe scrotal pain (especially in adolescents or young adults): go to ER immediately
- High fever with scrotal swelling: same-day evaluation for epididymo-orchitis or Fournier’s gangrene
- Scrotal skin changes (red, spreading, foul odor): emergency evaluation
- New varicocele with flank pain or blood in urine: urgent renal imaging needed
FAQ: Varicocele vs. Epididymitis
Can epididymitis cause long-term fertility problems like varicocele does?
Severe or recurrent epididymitis can cause epididymal obstruction, blocking sperm transport and potentially causing obstructive azoospermia. This is a different mechanism than varicocele-related fertility impairment (which is primarily from heat and oxidative stress). Both conditions can reduce fertility if untreated, but through distinct pathways requiring different evaluation and management strategies.
How can I tell at home whether I have varicocele or epididymitis?
Home self-assessment is limited but informative. Varicocele veins are typically felt as soft, non-tender cord-like structures above the testicle that enlarge when standing and reduce when lying down. Epididymitis produces a swollen, tender, warm area at the back of the testicle, often with fever and urinary symptoms. Neither replaces a clinical exam and ultrasound.
My doctor said I have chronic epididymitis but antibiotics didn’t help. Could it be varicocele?
Antibiotic-resistant chronic epididymitis that doesn’t respond to treatment is frequently misdiagnosed or co-exists with other causes of chronic scrotal pain, including varicocele. Request a scrotal Doppler ultrasound if you haven’t had one. A comparison of varicocele with other scrotal conditions may also help clarify your diagnosis before your next appointment.
Related Articles
Choose Varicocele Support Designed for Cooling, Lift, and Daily Comfort
You’ve seen why regular underwear often falls short. Now view the purpose-built option made to reduce heaviness, improve support, and feel comfortable enough for everyday wear.

