You’ve had a physical exam and your doctor found nothing. Your scrotal ultrasound came back borderline. Yet your semen analysis shows abnormal results, and your partner hasn’t conceived. Could a varicocele you can’t see or feel still be affecting your fertility? The answer is yes, and it goes by the name subclinical varicocele. This article explains what subclinical varicocele is, how it affects sperm without producing obvious symptoms, and what current evidence says about treatment versus watchful waiting. This is especially relevant if you’re in an unexplained infertility workup.
What Is a Subclinical Varicocele?
A subclinical varicocele is one that cannot be detected by physical examination alone but is visible on color Doppler ultrasound or venography. By definition, it produces no palpable varicose veins and causes no obvious scrotal symptoms. It sits one tier below a Grade 1 varicocele in the clinical classification system used by urologists and fertility specialists.
The diagnostic threshold for subclinical varicocele on Doppler ultrasound is retrograde blood flow in the pampiniform plexus with venous diameter under 2.5-3mm during the Valsalva maneuver. This is a subtle finding that requires experienced sonographers and proper technique to detect reliably. Understanding varicocele grades and severity helps frame where subclinical varicocele sits in the diagnostic spectrum.
Does Subclinical Varicocele Affect Sperm Quality?
This is one of the most debated questions in male reproductive medicine. The honest answer is: it can, but not always, and the effect size is smaller than with clinical varicocele. The primary mechanism of sperm damage is the same as in clinical varicocele: elevated scrotal temperature from impaired venous drainage, oxidative stress, and disrupted testicular thermoregulation.
A 2016 meta-analysis published in Fertility and Sterility found that men with subclinical varicocele had measurably lower total motile sperm counts and higher sperm DNA fragmentation rates compared to controls, though differences were less pronounced than in men with Grade 2-3 clinical varicoceles. This suggests a dose-response relationship: the larger the varicocele and the greater the venous reflux, the more sperm damage occurs, but even subclinical cases aren’t benign.
| Varicocele Type | Detectable by Exam | Doppler Reflux | Sperm DNA Fragmentation Risk |
|---|---|---|---|
| Subclinical | No | Present on Valsalva | Mildly elevated |
| Grade 1 (Clinical) | Only on Valsalva | Present | Moderately elevated |
| Grade 2 | Palpable at rest | Prominent | Elevated |
| Grade 3 | Visible without exam | Severe | Significantly elevated |
Sperm DNA Fragmentation: The Hidden Fertility Threat
Standard semen analysis (count, motility, morphology) can look relatively normal even in men with subclinical varicocele and significant fertility impairment. The missing piece is often sperm DNA fragmentation (SDF), which measures breaks and damage within sperm DNA strands. High SDF is associated with failed IVF cycles, recurrent miscarriage, and poor embryo development, none of which show up on a basic sperm count.
Men with subclinical varicocele often have elevated SDF as a primary finding. Research shows heat stress on the testis is a primary driver of DNA strand breaks in sperm. This is why varicocele’s impact on semen analysis and DNA fragmentation deserves targeted testing beyond a routine semen panel. If you’re pursuing assisted reproduction, ask your reproductive endocrinologist specifically about SDF testing.
Should Subclinical Varicocele Be Treated?
Current guidelines from the American Urological Association (AUA) and the American Society for Reproductive Medicine (ASRM) do not recommend routine treatment of subclinical varicocele. The position is that evidence for benefit in the subclinical group is insufficient to justify the risks and costs of intervention. This is a conservative stance that not all reproductive urologists agree with.
Where the picture shifts is in couples with documented infertility, abnormal semen parameters, elevated SDF, and a subclinical varicocele as the only identifiable male factor. In this specific scenario, some high-volume reproductive urologists will offer microsurgical varicocelectomy and report meaningful improvements in SDF and natural conception rates. Meta-analyses of varicocelectomy and pregnancy rates consistently show benefit in men with clinical varicocele and abnormal semen, with less data but emerging positivity for the subclinical group.
Conservative Approaches for Subclinical Varicocele
Even if surgery isn’t indicated, there are evidence-based steps men with subclinical varicocele can take to protect sperm quality:
- Scrotal cooling – avoid hot baths, saunas, laptops on the lap; wear cooling-supportive underwear
- Antioxidant supplementation – CoQ10, vitamin C, vitamin E, and L-carnitine have shown reduction in SDF in varicocele patients
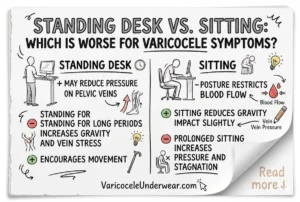
- Avoid prolonged sitting – increases scrotal temperature significantly
- Maintain healthy weight – obesity independently elevates scrotal temperature and SDF
- Regular ejaculation – reduces accumulation of oxidatively damaged sperm
Heat stress and fertility in varicocele is a well-documented relationship; mitigating thermal damage is one of the most practical non-surgical interventions available. Wearing cooling and supportive varicocele underwear consistently reduces ambient scrotal temperature and may help protect sperm quality over time.
Targeted fertility supplements for varicocele are also worth discussing with a reproductive urologist, particularly if you’re not a surgical candidate or are planning IVF in the near term.
FAQ: Subclinical Varicocele and Fertility
Can a normal physical exam rule out varicocele as a fertility cause?
No. Physical exam misses subclinical varicocele by definition. If you have unexplained infertility, abnormal semen parameters, or elevated sperm DNA fragmentation with a normal exam, request a color Doppler ultrasound with Valsalva maneuver. This is the only reliable way to detect subclinical venous reflux.
Will treating subclinical varicocele improve IVF success rates?
Evidence is emerging but not definitive. Some studies show that varicocelectomy in men with high sperm DNA fragmentation (from subclinical varicocele) improves ICSI outcomes, particularly reducing miscarriage rates. Discuss SDF testing and subspecialty referral with your reproductive endocrinologist if standard IVF cycles have failed.
Is subclinical varicocele permanent?
Subclinical varicocele can remain stable for years or progress to a clinically palpable grade over time, particularly with prolonged standing, heavy lifting, or increased intra-abdominal pressure. Annual Doppler monitoring is reasonable for men with subclinical varicocele and active fertility concerns. Lifestyle changes that reduce venous pressure may slow progression.