You’ve been told you have a varicocele. The aching in your scrotum makes sense on paper. But what if the pain persists even after treatment, or never quite matches the severity of your imaging results? There’s a real possibility that tight or dysfunctional pelvic floor muscles are either mimicking varicocele pain or making it significantly worse. This article breaks down the relationship between pelvic floor dysfunction and scrotal pain, who’s at risk, how to tell the difference, and what you can do about it. If you’ve been frustrated by pain that doesn’t add up, this is for you.
What Is Pelvic Floor Dysfunction in Men?
The pelvic floor is a group of muscles and connective tissue that stretches across the base of your pelvis. In men, these muscles support the bladder, bowel, and — critically — the scrotal contents and perineum. When these muscles become too tight, weakened, or poorly coordinated, the result is pelvic floor dysfunction (PFD).
PFD in men is underdiagnosed. Many urologists focus on structural causes of scrotal pain (varicocele, epididymitis, hydrocele) and overlook the muscular component entirely. Studies suggest that up to 31% of men with chronic scrotal pain have a pelvic floor component that is either contributing to or directly causing their symptoms.
How Pelvic Floor Muscles Mimic Varicocele Pain
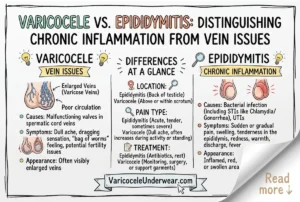
Varicocele pain is typically described as a dull, heavy ache in the left testicle that worsens after standing or physical activity and improves when lying down. Interestingly, hypertonic (overly tight) pelvic floor muscles produce nearly identical symptoms. The pudendal nerve, which runs through the pelvic floor and innervates the scrotum, can become compressed or irritated by tight muscles, generating referred pain that feels exactly like testicular or scrotal aching.
This is why some men get a varicocele repair and still experience the same pain afterward. The structural problem was fixed, but the muscular dysfunction was never addressed. In clinical practice, this scenario is more common than most patients realize. A 2017 study published in Translational Andrology and Urology noted that chronic orchialgia (testicular pain) frequently has a musculoskeletal origin that goes untreated.
| Symptom | Varicocele Pain | Pelvic Floor Dysfunction |
|---|---|---|
| Location | Left scrotum, testicle | Scrotum, perineum, inner thigh |
| Quality | Dull, heavy ache | Burning, aching, pressure |
| Worsens with | Standing, exertion | Sitting, stress, exertion |
| Improves with | Lying down | Relaxation, warm bath |
| Associated symptoms | Visible veins, fertility issues | Urinary urgency, painful sex |
Key Risk Factors for Pelvic Floor Dysfunction Alongside Varicocele
- Prolonged sitting (desk work, driving)
- High-intensity exercise without adequate recovery
- History of pelvic or abdominal surgery
- Chronic stress and anxiety (pelvic muscles hold tension)
- Previous scrotal trauma or hernia repair
- Constipation and straining
Men who do high-intensity interval training without proper form or recovery are particularly prone to developing pelvic floor tension that compounds existing varicocele discomfort.
Can Pelvic Floor Tension Actually Worsen a Varicocele?
This is a nuanced question. Pelvic floor tension does not cause varicocele (which is a venous valve problem), but it can impair venous return from the pelvic region. When pelvic muscles are chronically tight, they can compress pelvic veins and increase venous pressure in the region. This added pressure may worsen blood pooling in already-dilated spermatic veins. Think of it as a secondary amplifier of an existing problem.
Additionally, chronic pelvic tension activates pain sensitization pathways. Over time, the nervous system becomes hyperresponsive to stimuli in that region, meaning even mild venous engorgement triggers disproportionate pain. This is called central sensitization, and it is a known mechanism in chronic pelvic pain syndromes.
How Is Pelvic Floor Dysfunction Diagnosed?
Diagnosis typically involves a combination of clinical assessment and physical therapy evaluation. A pelvic floor physical therapist (PFPT) can assess muscle tone, trigger points, and coordination through external and internal examination techniques. Your urologist may also order a Doppler ultrasound to confirm or rule out active varicocele, ensuring both conditions are addressed.
- Detailed symptom mapping – noting exact location, triggers, and quality of pain
- Pelvic floor physical therapy assessment – muscle tone, trigger point identification
- Scrotal Doppler ultrasound – to confirm varicocele presence and grade
- Urodynamic testing – if urinary symptoms are present
- Pudendal nerve evaluation – in refractory cases
Treatment: Addressing Both Conditions Together
If you have both a varicocele and pelvic floor dysfunction, treating only one is likely to leave you with residual pain. The most effective approach combines varicocele management (whether conservative or surgical) with targeted pelvic floor physical therapy. Research consistently shows that men who receive multimodal treatment for chronic scrotal pain report better outcomes than those treated for a single structural cause.
Pelvic floor physical therapy for hypertonic muscles focuses on relaxation and lengthening rather than strengthening. Techniques include manual trigger point release, diaphragmatic breathing, biofeedback, and progressive muscle relaxation. Most patients see measurable improvement within 6-12 weeks of consistent therapy.
For symptomatic relief during recovery, properly fitted supportive underwear reduces scrotal movement and venous pressure. Options like the varicocele support underwear provide gentle scrotal lift that can reduce both vascular and musculoskeletal pain signals throughout the day.
Some men also benefit from acupuncture for varicocele pain, which has shown preliminary evidence for reducing pelvic and scrotal discomfort through neuromuscular pathways.
When to See a Specialist
See a urologist and a pelvic floor physical therapist if your scrotal pain persists beyond 3 months, doesn’t correlate with varicocele grade on imaging, returns after varicocele treatment, or is accompanied by perineal pressure, urinary urgency, or pain with sitting. These are red flags for an overlapping pelvic floor component that needs direct attention.
The pattern of your varicocele pain (sharp vs. dull, constant vs. intermittent) provides important diagnostic clues that both your urologist and physical therapist will want to know.
FAQ: Varicocele and Pelvic Floor Dysfunction
Can pelvic floor exercises make varicocele pain worse?
Standard Kegel exercises (pelvic floor contractions) can worsen pain if your pelvic floor is already too tight. In hypertonic PFD, you need muscle relaxation, not strengthening. Always get assessed by a pelvic floor physical therapist before starting any pelvic exercise program alongside a varicocele diagnosis.
How do I know if my scrotal pain is from varicocele or pelvic floor dysfunction?
Pain that worsens specifically with sitting, is accompanied by perineal pressure or urinary urgency, and doesn’t fully improve when lying down points more toward pelvic floor involvement. Varicocele pain classically improves significantly with recumbency. A Doppler ultrasound combined with a physical therapy assessment gives the clearest diagnostic picture.
Is pelvic floor dysfunction common after varicocele surgery?
Post-surgical pelvic floor tension is a recognized but underreported phenomenon. Surgical stress, altered movement patterns during recovery, and anxiety can all trigger protective muscle guarding in the pelvic region. Men who experience persistent pain after varicocele surgery or embolization should ask specifically about pelvic floor evaluation.