Most varicoceles develop slowly during adolescence and remain stable for years. But what happens when a varicocele appears suddenly in an adult man with no prior history? Or when it shows up on the right side, fails to decompress when lying down, or comes with other unexplained symptoms? These are not routine findings. Sudden-onset varicocele is a recognized red flag in urology for underlying pathology, most critically renal cell carcinoma (kidney cancer) or nutcracker syndrome. This article explains who needs urgent evaluation, what tests to request, and what the science says about the kidney-varicocele connection.
Why Sudden Varicocele Onset Is a Red Flag
Typical varicocele develops gradually due to faulty venous valves in the spermatic vein, most often on the left side. Sudden onset in an adult, particularly after age 35-40, suggests something is obstructing venous drainage from above rather than simple valve incompetence. The most feared cause is a renal tumor extending into the left renal vein and blocking the testicular vein outflow.
According to urological guidelines, a varicocele that does not empty when the patient lies down (a “non-reducible” or “standing” varicocele) warrants abdominal and renal imaging. This is a clinical rule taught in medical schools worldwide and reinforced by AUA male infertility guidelines.
The Anatomy: How a Kidney Tumor Causes a Varicocele
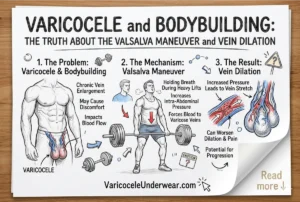
The left testicular vein drains directly into the left renal vein before emptying into the inferior vena cava (IVC). If a renal cell carcinoma (RCC) grows into the left renal vein as a tumor thrombus, it obstructs the testicular vein outflow, causing rapid engorgement of the pampiniform plexus. This is why left-sided sudden varicocele is the classic presentation in men with RCC.
Right-sided varicoceles are less common because the right testicular vein drains directly into the IVC at a favorable angle. A right-sided varicocele appearing de novo is even more alarming and should prompt immediate retroperitoneal and renal imaging to rule out IVC obstruction or right-sided renal pathology.
| Feature | Typical Varicocele | Secondary (Pathological) Varicocele |
|---|---|---|
| Onset | Gradual (adolescence) | Sudden (adult) |
| Side | Left (90%) | Right or bilateral |
| Reduces when lying down | Yes | No (non-reducible) |
| Age at presentation | Teens to 30s | 35+ (new onset) |
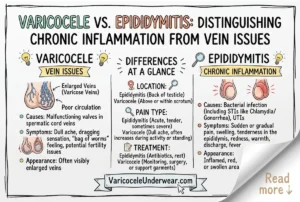
| Associated symptoms | Dull ache, fertility issues | Flank pain, hematuria, weight loss |
Renal Cell Carcinoma and Varicocele: What the Data Says
Renal cell carcinoma accounts for approximately 90% of kidney cancers and is among the most common urological malignancies. Studies estimate that venous tumor thrombus extension occurs in 4-10% of RCC cases, and in a subset of these, varicocele is the presenting symptom that leads to cancer diagnosis. This means the varicocele, in those cases, is not the disease but rather a symptom pointing to something more serious.
Early detection of RCC through this varicocele-triggered workup has been documented to improve patient outcomes significantly. Several case reports describe adult men presenting to fertility clinics or urologists for a new varicocele who were incidentally diagnosed with early-stage renal tumors. In some cases, the varicocele was the only symptom.
Other Causes of Secondary Varicocele
Kidney cancer is the most critical cause, but not the only one. Any mass or condition compressing pelvic or retroperitoneal veins can trigger secondary varicocele:
- Retroperitoneal lymphoma or sarcoma compressing the renal vein
- Nutcracker syndrome (aorto-mesenteric compression of the left renal vein)
- Renal vein thrombosis
- Large abdominal aortic aneurysm
- Retroperitoneal fibrosis
All of these conditions share one feature: they impair venous drainage upstream of the testicular vein. This is why imaging the entire retroperitoneum, not just the scrotum, is essential in sudden-onset varicocele cases.
Diagnostic Workup for Sudden-Onset Varicocele
If you or your doctor suspects a secondary varicocele, here is the standard diagnostic approach:
- Scrotal Doppler ultrasound – confirms varicocele, grades severity, assesses reflux pattern
- Renal and abdominal ultrasound – first-line screening for kidney mass or venous obstruction
- CT scan with contrast (CT urogram) – gold standard for renal tumor staging and vascular involvement
- MRI of abdomen/pelvis – preferred for soft tissue characterization, especially venous thrombus
- Urinalysis – screens for hematuria (blood in urine), a common RCC symptom
Do not delay imaging. A sudden adult-onset varicocele that doesn’t reduce in the lying position should be considered a potential oncological emergency until proven otherwise.
Red Flag Symptoms: When to Go to the ER
- Sudden, new varicocele in a man over 35 with no prior history
- Right-sided varicocele appearing de novo
- Varicocele that remains engorged and painful when lying flat
- Associated flank or back pain
- Blood in urine (hematuria)
- Unexplained weight loss or night sweats
- Palpable abdominal or flank mass
Any of these alongside a new varicocele warrants same-day or next-day evaluation, not a wait-and-see approach.
What Happens to the Varicocele After Kidney Treatment?
In secondary varicocele caused by renal tumor thrombus, surgical removal of the kidney and tumor (radical nephrectomy with thrombectomy) often resolves the varicocele entirely. The varicocele was a consequence of venous obstruction, so removing the obstruction eliminates the cause. This is another reason accurate diagnosis matters: treating the varicocele alone (with embolization or ligation) without addressing the underlying tumor would be medically dangerous.
For men managing chronic varicocele symptoms during diagnostic workup or conservative treatment, supportive varicocele underwear can reduce day-to-day scrotal discomfort while a definitive diagnosis is being established. Understanding the full scope of untreated varicocele long-term effects also helps patients communicate urgency to their healthcare providers.
FAQ: Sudden Onset Varicocele and Kidney Disease
Can a varicocele cause kidney problems, or is it the other way around?
In secondary varicocele, the kidney problem causes the varicocele, not the reverse. A renal tumor or venous obstruction blocks testicular vein drainage, leading to engorgement. Standard adolescent varicocele does not damage the kidneys. If you have a new adult-onset varicocele, kidney imaging is the priority.
How common is kidney cancer as a cause of varicocele?
It’s rare as a percentage of all varicoceles but significant enough that all guidelines recommend imaging for sudden-onset or non-reducible cases. In adult men presenting with new-onset left varicocele that doesn’t collapse when lying down, RCC is found in a meaningful minority of cases, making the workup non-negotiable from a clinical standpoint.
Should a teenager with a new varicocele get kidney imaging?
Adolescent varicoceles are almost always primary (valve-related) and rarely indicate underlying pathology. However, if the varicocele is right-sided, bilateral, or associated with other symptoms like hematuria or flank pain in any age group, renal imaging is appropriate. Routine adolescent varicocele does not typically require abdominal CT scanning.