If you’ve undergone varicocele surgery and notice familiar symptoms returning, you’re not imagining things. Varicocele recurrence is a real possibility that affects approximately 10% of men after surgical treatment. This guide will help you understand why varicoceles can come back, which surgical techniques have the lowest recurrence rates, and what treatment options exist if you’re facing this frustrating situation.
What Causes Varicocele to Come Back After Surgery?
Recurrence occurs when abnormal blood flow reappears in the testicular veins even after surgical correction. In such cases, understanding the links between varicocele and treatment outcomes becomes especially important, since repeated episodes can have a stronger impact on male reproductive health.
The Main Reasons for Varicocele Recurrence
Research identifies three primary causes of varicocele returning after surgery:
Incomplete vein ligation: The most common cause, accounting for approximately 60% of recurrences, occurs when not all problematic veins are identified and closed during surgery. Studies show that larger dilated veins are significantly associated with higher recurrence rates.
Collateral vein networks: Your body has extensive connections between the internal spermatic vein, vas deferens vein, external spermatic vein, and abdominal superficial veins. Blood can find alternate pathways through these interconnected networks, causing symptoms to return even after the main veins are tied off.
Underlying anatomical issues: Left renal vein entrapment (also called Nutcracker Syndrome) affects approximately 28% of varicocele patients. Men with this condition face a recurrence rate of 1.98% compared to just 0.05% in those without it, according to research analyzing over 3,000 patients.
Varicocele Recurrence Rates by Surgical Technique
Not all surgical approaches carry the same risk of recurrence. Here’s what current medical evidence shows:
| Surgical Technique | Recurrence Rate | Key Characteristics |
|---|---|---|
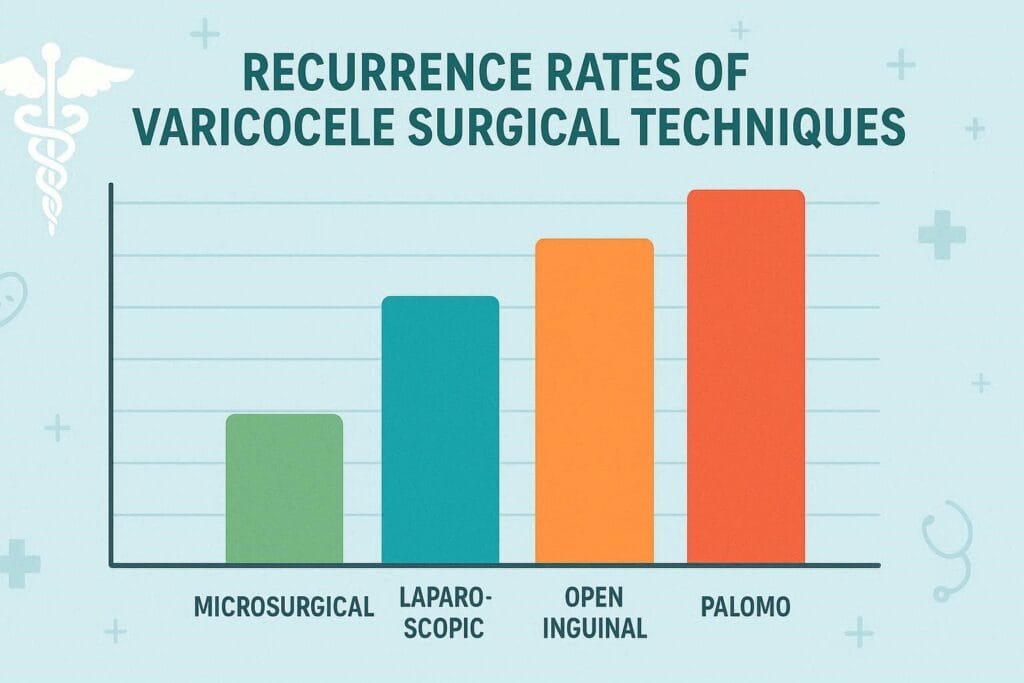
| Microsurgical (subinguinal/inguinal) | 0.6% to 2.9% | Lowest recurrence, uses magnification to identify all veins |
| Open inguinal varicocelectomy | Up to 15% | Most common approach, moderate recurrence risk |
| Laparoscopic varicocelectomy | 6% to 17.6% | Minimally invasive but higher recurrence than microsurgical |
| Open abdominal (Palomo) | Variable (higher) | Retroperitoneal approach, limited vein visualization |
Research consistently demonstrates that microsurgical techniques offer the lowest recurrence rates because surgeons can see and ligate all vein branches under magnification. However, even with the best surgical approach, recurrence remains possible.
Risk Factors That Increase Your Chances of Recurrence
Certain factors make some men more susceptible to varicocele returning after surgery:
Clinical Risk Factors
Higher varicocele grade: Men with Grade III varicoceles (the most severe) face increased recurrence risk compared to Grade I cases. The size of dilated veins matters significantly.
Lower body mass index (BMI): Research found that men with a BMI of 24.8 had higher recurrence rates compared to those with a BMI of 26.9. Each one-unit decrease in BMI correlates with a 1.25 times increased recurrence risk.
Larger vein diameter: Studies indicate that the diameter of the left spermatic vein during Valsalva maneuver strongly predicts recurrence likelihood.
Left renal vein entrapment: This anatomical variation dramatically increases recurrence risk and should be evaluated before surgery using Doppler ultrasound.
Timeline for Recurrence
Most varicocele recurrences become apparent within the first year after surgery. Research tracking recurrent cases found the average time to recurrence was 5.3 months, with a range from less than one month to 13 months after the initial procedure.
Discover specialized varicocele underwear designed for daily comfort, support, and recovery — a more targeted option for men who want support without compromise.
Discover the Recommended OptionRecognizing Recurrent Varicocele Symptoms
You might be dealing with a recurrence if you notice:
- Return of the “bag of worms” feeling in your scrotum
- Renewed testicular or scrotal pain, especially after standing
- Visible or palpable enlarged veins in the scrotum
- Changes in testicular size (the affected testicle may shrink)
- Worsening semen parameters if you’re tracking fertility
Your doctor will diagnose recurrence through physical examination combined with Doppler ultrasound, which can detect blood flow patterns that indicate the varicocele has returned.
Treatment Options for Recurrent Varicocele
Discovering your varicocele has returned doesn’t mean you’re back to square one. You have effective treatment options, and the good news is that managing recurrent varicoceles often yields excellent results.
Varicocele Embolization: The Preferred Option for Recurrence
Most specialists now recommend embolization as the first-line treatment for recurrent varicocele. This minimally invasive procedure has several advantages over repeat surgery:
How it works: An interventional radiologist inserts a thin catheter through a small nick in your groin or neck. Using real-time X-ray imaging, they navigate to the affected veins and block them with tiny coils or a sclerosing solution. This redirects blood flow to healthy veins.
Success rates: Recent research following patients for 15 years found that embolization achieved 96% technical success and 93.75% clinical success, with only 6.25% confirmed recurrence on ultrasound.
Recovery advantages:
- 1-2 days recovery time (versus 2-3 weeks for surgery)
- Resume sexual activity in 2 weeks (versus 4 weeks post-surgery)
- No surgical incisions or scarring
- Can be performed with local anesthesia and sedation
- Treats bilateral varicoceles in one session
Why embolization works better for recurrence: Embolization allows doctors to precisely identify which veins are causing the problem through venography. Studies show that 64% of recurrent varicoceles involve patent internal spermatic veins that can be effectively treated with embolization.
Repeat Microsurgical Repair
If embolization isn’t suitable or wasn’t successful, repeat microsurgical varicocelectomy remains an option. Research indicates that 83% of patients who had recurrence after initial microsurgical repair successfully underwent repeat microsurgical surgery.
Considerations for repeat surgery:
- Best performed by experienced microsurgeons
- Higher complexity due to scar tissue from previous surgery
- May require a different surgical approach than the initial operation
- Still carries a small risk of another recurrence
Comparative Outcomes: Surgery vs. Embolization for Recurrence
Systematic review data comparing treatment methods for recurrent varicocele found:
| Outcome Measure | Surgical Methods | Embolization |
|---|---|---|
| Spontaneous pregnancy rate | 44.3% | 17.9% |
| Sperm parameter improvement | 77.5% | 62.5% |
| Post-treatment recurrence | 3.8% (microsurgical: 0.6%) | 3.3% |
| Technical failure | Very low | 11.8% |
While surgery shows higher pregnancy rates, embolization offers faster recovery and is less invasive. Your specific situation, anatomical factors, and the type of initial surgery you had should guide your decision.
Managing Symptoms While Considering Treatment
Whether you’re weighing treatment options or have already scheduled a procedure, managing daily discomfort remains important. Many men find relief through supportive measures:

Supportive underwear: Specialized varicocele support underwear provides gentle elevation and cooling that can reduce discomfort. This non-invasive approach helps many men manage symptoms between diagnosis and treatment or during recovery.
Lifestyle modifications:
- Avoid prolonged standing or heavy lifting when possible
- Apply ice packs to reduce swelling and discomfort
- Take over-the-counter pain relievers as needed
- Wear snug-fitting briefs for additional support
These measures won’t eliminate the varicocele but can make symptoms more manageable as you plan your next steps.
Making Informed Treatment Decisions
When facing recurrent varicocele, consider these questions with your healthcare provider:
- What caused the initial recurrence? Understanding whether incomplete ligation, collateral veins, or anatomical factors contributed helps determine the best approach.
- Do you have left renal vein entrapment? If not evaluated before your first surgery, request Doppler ultrasound to check for this condition.
- What’s your primary concern? Pain relief typically responds well to either treatment, while fertility concerns might influence your choice between surgery and embolization.
- Is embolization available in your area? Not all facilities offer this specialized procedure, though availability has increased significantly.
- What’s your surgeon or interventional radiologist’s experience? Outcomes improve with practitioner experience, especially for complex recurrent cases.
Preventing Future Recurrence
While you can’t control anatomical factors like vein anatomy or left renal vein entrapment, choosing the most appropriate treatment approach the first time matters. Evidence shows microsurgical techniques offer the lowest recurrence rates for initial treatment.
For recurrent cases, thorough preoperative evaluation including venography or detailed Doppler ultrasound helps identify all problem veins, reducing the chance of another recurrence.
The Bottom Line
Yes, varicoceles can return after surgery, with approximately 10% of men experiencing recurrence. The likelihood depends heavily on the surgical technique used, your individual anatomy, and risk factors like varicocele grade and left renal vein entrapment.
Modern medicine offers excellent treatment options for recurrent varicoceles, with embolization emerging as the preferred first-line approach due to its high success rate, minimal invasiveness, and rapid recovery. Whether you choose embolization or repeat surgery, working with experienced specialists and ensuring thorough preoperative evaluation gives you the best chance of successful, lasting treatment.
If you’re experiencing symptoms that suggest your varicocele has returned, don’t delay seeking evaluation. Early intervention can prevent symptom progression and protect your fertility potential.
Frequently Asked Questions
How long after varicocele surgery should I worry about recurrence?
Most recurrences become apparent within 6-12 months after surgery, with an average of 5.3 months. However, late recurrences can occur beyond the first year. If you notice returning symptoms at any point after surgery, schedule an evaluation with your doctor. Regular follow-up appointments during the first year help catch recurrence early when it’s most treatable.
Can varicocele recur after embolization treatment?
Yes, though the recurrence rate after embolization is comparable to or lower than surgery. Recent studies report actual recurrence rates of 3.3% to 6.25% based on ultrasound confirmation, though patients sometimes report higher rates (up to 25%) based on symptoms alone. If recurrence happens after embolization, repeat embolization succeeds in approximately 87% of cases. The procedure can be safely repeated because it doesn’t create scar tissue like surgery does.
Does varicocele grade affect how likely it is to come back?
Absolutely. Higher-grade varicoceles (Grade II and III) have significantly higher recurrence rates than Grade I cases. Research shows that advanced varicocele grade on the left side, combined with larger vein diameter, strongly predicts recurrence. If you had a high-grade varicocele initially, microsurgical repair or embolization offers better protection against recurrence than open surgical techniques. Discuss your specific grade with your doctor when choosing between treatment options.
Related Articles
Choose Varicocele Support Designed for Cooling, Lift, and Daily Comfort
You’ve seen why regular underwear often falls short. Now view the purpose-built option made to reduce heaviness, improve support, and feel comfortable enough for everyday wear.

