Fertility supplements for varicocele are one of the most searched topics in male reproductive health, and also one of the most poorly regulated markets. For every well-studied compound with genuine evidence, there are a dozen overpriced proprietary blends with zero clinical data. This independent 2026 review covers the ten supplements with the strongest evidence specifically for varicocele-related male infertility, breaking down what each does mechanistically, what the clinical data shows, realistic dosing, and which combinations are worth considering. No supplement cures varicocele. But several have genuine evidence for reducing the oxidative stress and sperm DNA damage that varicocele causes.
Why Antioxidants Are Central to Varicocele Supplement Strategy
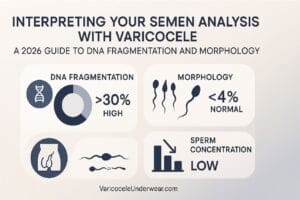
Varicocele damages sperm through two primary mechanisms: elevated scrotal temperature and reactive oxygen species (ROS) overproduction from pooled venous blood. The oxidative stress pathway is where supplements have the most direct mechanistic relevance. When ROS levels exceed the testis’s antioxidant defenses, sperm DNA fragmentation increases, motility decreases, and morphology deteriorates. Antioxidant supplementation raises the antioxidant capacity of seminal plasma and spermatogenic tissue, directly countering this mechanism.
A 2025 study published in Clinical and Experimental Reproductive Medicine demonstrated that oral antioxidant supplementation in infertile men with varicocele improved sperm parameters and sperm DNA fragmentation comparably to varicocele surgery in some patient subgroups, underscoring the biological relevance of the oxidative pathway and the genuine therapeutic potential of well-chosen antioxidants. This doesn’t replace surgery for men who need it, but it validates supplementation as a legitimate treatment adjunct.
The Top 10 Supplements: Evidence and Dosing
1. Coenzyme Q10 (CoQ10 / Ubiquinol)
CoQ10 is a mitochondrial cofactor and potent antioxidant concentrated in sperm midpiece mitochondria. Multiple randomized controlled trials show supplementation increases sperm motility, concentration, and morphology in men with oligoasthenoteratospermia, with effects particularly pronounced in men with high baseline oxidative stress (as in varicocele). A 2012 RCT demonstrated significant improvement in all three main semen parameters after 26 weeks of 300mg/day CoQ10. The ubiquinol form (reduced CoQ10) is better absorbed than ubiquinone, particularly in men over 35.
- Evidence level: Strong (multiple RCTs)
- Dose: 200-400mg/day ubiquinol with fat-containing meal
- Primary effect: sperm motility, mitochondrial energy production, DNA protection
- Timeline to effect: 12-26 weeks
2. L-Carnitine / Acetyl-L-Carnitine
L-Carnitine is concentrated in the epididymis and plays a central role in sperm energy metabolism and motility. It facilitates fatty acid transport into mitochondria for ATP production. Combined L-carnitine and acetyl-L-carnitine supplementation has shown consistent improvement in sperm motility in multiple controlled studies. A meta-analysis of L-carnitine supplementation in male infertility found statistically significant improvements in sperm concentration and motility with good safety profiles.
- Evidence level: Strong (meta-analysis level)
- Dose: L-carnitine 2g/day + Acetyl-L-carnitine 1g/day (combination)
- Primary effect: sperm motility, progressive forward movement
- Timeline to effect: 12-24 weeks
3. Vitamin C (Ascorbic Acid)
Vitamin C is the predominant water-soluble antioxidant in seminal plasma, present at concentrations 10x higher than in blood plasma. It directly neutralizes ROS, protects sperm DNA from oxidative strand breaks, and regenerates vitamin E after it donates electrons. Studies in men with varicocele specifically show that vitamin C supplementation reduces sperm DNA fragmentation and improves seminal oxidative stress markers. It is one of the lowest-cost, most bioavailable, and best-studied options in the fertility supplement space.
Discover specialized varicocele underwear designed for daily comfort, support, and recovery — a more targeted option for men who want support without compromise.
Discover the Recommended Option- Evidence level: Good (multiple clinical studies)
- Dose: 500-1000mg/day (split dosing reduces GI side effects)
- Primary effect: DNA fragmentation reduction, seminal ROS neutralization
- Timeline to effect: 8-16 weeks
4. Vitamin E (Mixed Tocopherols)
The primary fat-soluble antioxidant in cell membranes, vitamin E protects sperm plasma membranes from lipid peroxidation, a process particularly active in varicocele patients where elevated ROS attacks the polyunsaturated fatty acid-rich sperm membranes. Vitamin E works synergistically with vitamin C (each regenerates the other), which is why combined C + E supplementation consistently outperforms either alone in clinical studies of male infertility.
- Evidence level: Good
- Dose: 400IU/day mixed tocopherols (avoid dl-alpha-tocopherol synthetic form)
- Primary effect: membrane protection, lipid peroxidation reduction
- Note: do not exceed 800IU/day; high-dose vitamin E has shown adverse cardiovascular effects in some studies
5. Zinc
Zinc is essential for testosterone synthesis, sperm development, and seminal fluid composition. It is the most abundant trace element in semen, and zinc deficiency directly impairs spermatogenesis. Men with varicocele often have lower seminal zinc concentrations than controls, and supplementation in zinc-deficient men with poor semen parameters consistently improves sperm count, motility, and morphology. Testing for zinc deficiency (serum zinc) before supplementing helps identify who benefits most.
- Evidence level: Strong for zinc-deficient men
- Dose: 25-50mg elemental zinc daily (zinc gluconate or zinc citrate forms have best absorption)
- Primary effect: testosterone support, sperm count and motility
- Note: balance with 1-2mg copper to prevent copper deficiency from chronic zinc use
6. Folate (Methylfolate) + Zinc Combination
The folate-zinc combination specifically targets sperm DNA integrity. Folate is a methyl donor essential for DNA synthesis and repair during spermatogenesis. Zinc supports folate metabolism. A landmark study found that combined zinc-folate supplementation increased total normal sperm count by 74% in subfertile men. For men with varicocele and high sperm DNA fragmentation, this combination addresses the DNA damage pathway more directly than most other supplements. Use methylfolate (5-MTHF) rather than folic acid if there is any possibility of MTHFR gene polymorphism.
- Evidence level: Good
- Dose: 400-800mcg methylfolate/day + zinc as above
- Primary effect: sperm DNA integrity, total normal sperm count
7. Selenium
Selenium is a cofactor for glutathione peroxidase, the primary endogenous antioxidant enzyme in sperm. GPx4, the selenium-dependent isoform, is structurally incorporated into the sperm midpiece and is essential for sperm motility and structural integrity. Low selenium is associated with increased sperm DNA fragmentation and reduced motility. Selenium combined with vitamin E has shown synergistic improvement in sperm motility in men with idiopathic infertility and varicocele-related infertility.
- Evidence level: Good
- Dose: 100-200mcg/day selenomethionine form
- Note: do not exceed 400mcg/day; selenium toxicity (selenosis) occurs with over-supplementation
- Primary effect: sperm motility, structural integrity via GPx4
8. Lycopene
Lycopene is a carotenoid antioxidant found in high concentrations in the testis and seminal plasma. It has demonstrated specific efficacy in men with idiopathic infertility and varicocele: a double-blind RCT found that lycopene supplementation at 4mg twice daily for 3 months significantly improved sperm concentration and motility, with the effect most pronounced in men with existing oxidative stress markers. Lycopene also has anti-inflammatory properties relevant to the venous wall inflammation that characterizes varicocele.

- Evidence level: Moderate-Good (RCT data)
- Dose: 4mg twice daily with meals (fat-soluble; take with fat-containing food)
- Primary effect: sperm concentration and motility, anti-inflammatory vascular support
9. N-Acetyl Cysteine (NAC)
NAC is a precursor to glutathione, the most important intracellular antioxidant. It directly replenishes glutathione stores in testicular tissue depleted by the chronic oxidative stress of varicocele. Multiple clinical studies specifically in men with varicocele show that NAC supplementation reduces seminal ROS, improves sperm motility, and reduces sperm DNA fragmentation. It is fast-acting relative to other antioxidants, with measurable changes in oxidative stress markers within 4-8 weeks.
- Evidence level: Good (varicocele-specific studies)
- Dose: 600mg twice daily
- Primary effect: glutathione replenishment, rapid ROS reduction, DNA fragmentation
- Timeline to effect: 4-8 weeks (fastest in this list)
10. Omega-3 Fatty Acids (DHA/EPA)
DHA (docosahexaenoic acid) is the predominant fatty acid in sperm plasma membranes and is essential for membrane fluidity, which directly affects sperm motility and the acrosome reaction required for fertilization. Omega-3 supplementation in men with varicocele-related infertility has shown improvements in sperm total motility and morphology. EPA has additional anti-inflammatory effects on vascular endothelium that may specifically benefit the chronically inflamed venous walls of varicocele. Use a molecularly distilled, third-party-tested fish oil or algal DHA source.
- Evidence level: Moderate-Good
- Dose: 2-3g/day combined EPA+DHA (minimum 1g DHA)
- Primary effect: sperm membrane integrity, motility, anti-inflammatory vascular support
Practical Supplement Stack for Varicocele: 2026 Recommendations
Rather than taking all ten simultaneously (expensive and unnecessary), a practical tiered approach based on budget and specific deficiencies:
| Priority Tier | Supplements | Primary Target |
|---|---|---|
| Tier 1 (Core) | CoQ10 (ubiquinol) + NAC + Zinc + Vitamin C | ROS reduction, DNA fragmentation, motility |
| Tier 2 (Add-on) | L-Carnitine/Acetyl-L-Carnitine + Selenium + Vitamin E | Motility, membrane protection, antioxidant depth |
| Tier 3 (Optional) | Lycopene + DHA/EPA + Methylfolate | Anti-inflammatory, membrane integrity, DNA synthesis |
The full picture of varicocele’s effect on sperm DNA fragmentation and how to track improvement helps contextualize whether your supplement protocol is working: semen analysis at baseline and after a full 74-day spermatogenesis cycle is the only objective measure. Combine supplementation with thermal management through cooling varicocele underwear for a comprehensive conservative approach that addresses multiple damage mechanisms simultaneously.
FAQ: Fertility Supplements for Varicocele
Can supplements replace varicocele surgery for fertility?
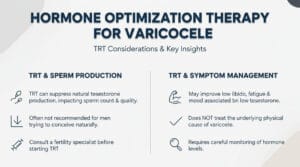
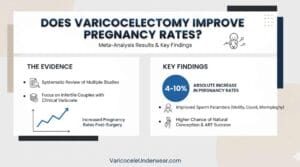
A 2025 study found antioxidant supplementation improved sperm parameters comparably to surgery in some varicocele patient subgroups. However, surgery produces more durable improvement by addressing the underlying anatomy, while supplements require continuous use to maintain effect. For men with clinical varicocele and significant fertility impairment, supplements are best used as an adjunct to, not a replacement for, appropriate surgical management. They are a valid first-line option for subclinical varicocele or when surgery is not yet indicated.
How long should I take fertility supplements before assessing response?
A minimum of 3 months (one full spermatogenesis cycle of 74 days, plus buffer) is required before repeating a semen analysis to assess supplement response. Stopping earlier gives an inaccurate picture. If starting supplements before varicocele surgery, begin at least 3 months pre-operatively to optimize sperm quality at the time of the procedure and continue through the post-operative period. The varicocele and fertility guide provides context for interpreting semen analysis improvements.
Are combined fertility supplement formulas (pre-made stacks) worth buying?
Pre-made male fertility formulas vary enormously in quality. Evaluate them against this checklist: does the product disclose the exact dose of each ingredient (not a “proprietary blend” that hides underdosing), does it include CoQ10 at 200mg+ per serving, does it use methylfolate rather than folic acid, and is it third-party tested for purity? Products that meet all four criteria are worth comparing to building your own stack. Most retail formulas underdose the most evidence-supported ingredients, making a custom stack more cost-effective at therapeutic doses.
Related Articles

Choose Varicocele Support Designed for Cooling, Lift, and Daily Comfort
You’ve seen why regular underwear often falls short. Now view the purpose-built option made to reduce heaviness, improve support, and feel comfortable enough for everyday wear.

