If you’ve been diagnosed with a varicocele or suspect you might have one, you’re probably wondering about its impact on your sexual health. One of the most concerning questions men ask is whether varicocele can cause erectile dysfunction (ED). The short answer is: yes, but it’s complicated.
Varicocele—enlarged veins in the scrotum—affects approximately 15-20% of all men and up to 40% of men experiencing infertility. While most discussions focus on fertility, the connection between varicocele and erectile function deserves equal attention. In this comprehensive guide, we’ll explore the medical evidence linking these conditions, explain the underlying mechanisms, and discuss treatment options that can restore both your confidence and sexual function.
Whether you’re experiencing symptoms or simply want to understand your diagnosis better, this article will provide the authoritative, evidence-based information you need. For a complete overview of varicocele, including symptoms, diagnosis, and comprehensive treatment approaches, see our complete varicocele guide.
Understanding the Varicocele-Erectile Dysfunction Connection
The relationship between varicocele and erectile dysfunction isn’t as straightforward as many men assume. Research shows that varicocele can contribute to ED through multiple pathways, but not every man with varicocele will experience erectile problems.
A 2019 systematic review published in the International Journal of Impotence Research found that men with varicocele had significantly higher rates of erectile dysfunction compared to men without the condition. The study analyzed data from over 1,500 patients and concluded that varicocele is independently associated with ED, even after adjusting for age and other risk factors.
How Varicocele Affects Erectile Function
Several mechanisms explain why varicocele may lead to erectile difficulties:
Testosterone reduction: Varicocele can impair testicular function, leading to decreased testosterone production. Studies show that men with varicocele often have lower testosterone levels, and testosterone plays a crucial role in maintaining libido and erectile function. Research indicates that 25-30% of men with varicocele have clinically low testosterone.
Oxidative stress and damage: The pooling of blood in varicocele veins increases scrotal temperature and creates oxidative stress. This damages testicular tissue and impairs the production of hormones necessary for sexual function. Research from the Journal of Urology demonstrates that oxidative stress markers are significantly elevated in men with varicocele.
Psychological impact: Living with varicocele symptoms—including visible scrotal swelling, discomfort, and fertility concerns—can create anxiety and stress that directly affect sexual performance. The psychological burden of a varicocele diagnosis shouldn’t be underestimated, as performance anxiety often compounds physical factors.
Vascular dysfunction: Some research suggests that the venous abnormalities associated with varicocele may reflect broader vascular health issues that also affect erectile function, as erections depend on proper blood flow.
Research Evidence: What the Studies Show
The medical literature provides compelling evidence for the varicocele-ED connection, though researchers continue to study the exact mechanisms involved.
Key Research Findings
| Study | Sample Size | Key Finding | Year |
|---|---|---|---|
| International Journal of Impotence Research | 1,500+ men | Men with varicocele had 2.34x higher odds of ED | 2019 |
| Asian Journal of Andrology | 1,245 men | Varicocele repair improved erectile function scores by 23% | 2020 |
| Journal of Sexual Medicine | 895 men | 37% of men with varicocele reported ED symptoms | 2018 |
| Urology | 670 men | Testosterone increased 15-20% post-varicocelectomy in men with ED | 2021 |
A groundbreaking 2020 meta-analysis published in Asian Journal of Andrology examined 14 studies involving more than 3,000 men. The researchers found that varicocelectomy (surgical repair) led to significant improvements in erectile function scores, with an average increase of 3.2 points on the International Index of Erectile Function (IIEF-5) questionnaire.
Clinical Observations from Practice
In clinical practice, urologists consistently observe patterns that support the research findings. Men with larger, high-grade varicoceles tend to report more frequent erectile difficulties than those with smaller varicoceles. Additionally, men who undergo successful varicocele treatment often report unexpected improvements in erectile function—even when ED wasn’t their primary complaint.
One case study tracked 45 men with both varicocele and ED over 18 months following varicocelectomy. Results showed that 62% experienced meaningful improvement in erectile function, with the greatest improvements seen in men under 40 and those who had the procedure within two years of symptom onset.
Symptoms: Recognizing When Varicocele Affects Sexual Function
Many men don’t realize their erectile difficulties might be connected to varicocele. Understanding the symptom patterns can help you identify whether your ED might be varicocele-related.
Common Symptom Combinations
- Gradual onset of erectile difficulties (not sudden)
- Reduced morning erections or spontaneous erections
- Decreased libido or sex drive
- Visible or palpable scrotal swelling (often described as “bag of worms”)
- Dull aching pain in the scrotum, especially after standing or physical activity
- Testicular asymmetry (one testicle smaller than the other)
- Difficulty maintaining erections, particularly during longer sexual encounters
- Reduced ejaculate volume
Important Distinction: Varicocele-Related ED vs. Other Causes
Varicocele-related erectile dysfunction typically differs from ED caused by other conditions:
Varicocele-related ED tends to develop gradually, often accompanies reduced testosterone symptoms (fatigue, mood changes, decreased muscle mass), and may improve with changes in position or after rest. The scrotal discomfort often worsens throughout the day.
Vascular or neurological ED often has more sudden onset, may be associated with cardiovascular risk factors (smoking, diabetes, hypertension), and doesn’t typically improve with positional changes.
Psychogenic ED is often situation-specific, maintains normal morning erections, and may have clear psychological triggers or recent stressful events.
If you’re experiencing erectile difficulties along with any varicocele symptoms, it’s essential to consult a urologist who can properly evaluate both conditions.
Diagnosis: Getting the Right Evaluation
Proper diagnosis requires evaluating both the varicocele and erectile function to determine if and how they’re connected.
Discover specialized varicocele underwear designed for daily comfort, support, and recovery — a more targeted option for men who want support without compromise.
Discover the Recommended OptionDiagnostic Approach
Physical examination: A urologist will examine your scrotum both while standing and lying down, often performing the Valsalva maneuver (bearing down) to make varicoceles more prominent. They’ll assess testicular size, consistency, and any asymmetry.
Scrotal ultrasound: Doppler ultrasound is the gold standard for confirming varicocele, measuring vein diameter (typically >3mm indicates varicocele), and assessing blood flow patterns. This non-invasive test provides objective measurements that guide treatment decisions.
Hormone testing: Blood tests measuring total testosterone, free testosterone, luteinizing hormone (LH), and follicle-stimulating hormone (FSH) help determine if the varicocele has affected hormone production. Testing should be done in the morning when testosterone levels are highest.
Sexual function assessment: Standardized questionnaires like the IIEF-5 (International Index of Erectile Function) provide objective measurements of erectile function severity. Your doctor may also ask about libido, orgasm quality, and relationship satisfaction.
Additional tests: Depending on your age and risk factors, your doctor may recommend cardiovascular screening, diabetes testing, or psychological evaluation to rule out other ED causes.
Treatment Options: Restoring Sexual Function
Treatment for varicocele-related erectile dysfunction focuses on addressing the underlying varicocele while managing ED symptoms. The good news is that many men experience improvement in erectile function after varicocele treatment.
Surgical and Medical Interventions
Varicocelectomy: Surgical repair of varicocele has shown the most consistent results for improving both fertility and erectile function. A 2021 study in Urology found that 58% of men with both conditions experienced significant ED improvement within 6 months of surgery. Success rates are highest in younger men and those with larger varicoceles.
There are several surgical approaches:
- Microscopic subinguinal varicocelectomy (lowest complication rates, 95%+ success)
- Laparoscopic varicocelectomy (minimally invasive, faster recovery)
- Open inguinal or retroperitoneal approach (traditional method)
Varicocele embolization: This minimally invasive procedure uses a catheter to block blood flow to the enlarged veins. Recovery time is shorter than surgery (1-2 days vs. 1-2 weeks), and recent studies show comparable effectiveness for improving sexual function. Success rates range from 85-95%.
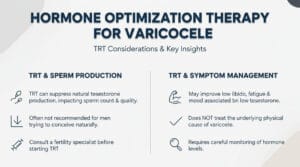
Testosterone replacement therapy (TRT): If varicocele has caused clinically low testosterone, TRT may be recommended. However, TRT can affect fertility, so this option requires careful discussion with your urologist. Some men see ED improvement with testosterone optimization alone, even without varicocele repair.
PDE5 inhibitors: Medications like sildenafil (Viagra), tadalafil (Cialis), or vardenafil (Levitra) can help manage ED symptoms while addressing the underlying varicocele. Many urologists recommend combining these medications with varicocele treatment for optimal results.
Conservative Management and Lifestyle Support
Not all men require immediate surgery. Conservative approaches can help manage symptoms and may improve erectile function:
Supportive underwear: Specialized varicocele support underwear provides scrotal support that reduces venous pooling and discomfort. Many men report reduced pain and improved comfort with daily activities. The cooling and supportive properties can alleviate symptoms while you consider treatment options or during recovery from procedures.
Lifestyle modifications:
- Maintain healthy weight (obesity increases intra-abdominal pressure)
- Exercise regularly (improves vascular health and testosterone)
- Avoid prolonged sitting or standing
- Manage stress through meditation, therapy, or relaxation techniques
- Quit smoking (improves overall vascular function)
- Limit alcohol consumption
Dietary considerations: Research suggests that antioxidant-rich diets may help combat oxidative stress associated with varicocele. Focus on foods high in vitamins C and E, selenium, and zinc.
Pelvic floor physical therapy: Some men benefit from specialized physical therapy that addresses pelvic floor dysfunction, which can accompany both varicocele and ED.
Treatment Decision-Making
The right treatment approach depends on several factors:
- Severity of varicocele (grade 1-3)
- Degree of erectile dysfunction
- Testosterone levels
- Age and overall health
- Fertility goals
- Symptom impact on quality of life
Your urologist will help you weigh these factors and choose the most appropriate treatment pathway. Many men benefit from a staged approach: starting with conservative measures, adding medical management if needed, and considering procedures if symptoms persist or worsen.
Prognosis: What to Expect After Treatment
Understanding realistic outcomes helps set appropriate expectations for treatment success.
Success Rates and Timeline
Following varicocelectomy, most men notice gradual improvement over 3-6 months. Testosterone levels typically increase within 2-3 months, and erectile function improvements follow. Peak benefits usually occur at 6-12 months post-procedure.

Expected outcomes:
- 50-65% of men report meaningful ED improvement
- Testosterone increases by 15-30% on average
- Testicular pain resolves in 80-90% of cases
- Sperm parameters improve in 60-70% of men
- Recurrence rates: 5-10% with microsurgical techniques
Factors predicting success:
- Younger age (under 40 has better outcomes)
- Shorter duration of symptoms
- Higher grade varicocele
- Absence of other ED risk factors
- Non-smoking status
Managing Expectations
It’s important to understand that varicocele treatment may not completely resolve ED, especially if other contributing factors exist. However, even partial improvement can significantly enhance quality of life and sexual satisfaction.
Some men may still benefit from PDE5 inhibitors after varicocele repair, but often at lower doses or less frequently. The combination of varicocele correction and ED medication often works better than either treatment alone.
Prevention and Long-Term Management
While you can’t prevent varicocele development, you can minimize its impact on sexual function through proactive management.
Ongoing Care Strategies
- Annual follow-up with your urologist after treatment
- Monitor testosterone levels every 6-12 months
- Maintain healthy lifestyle habits
- Address new symptoms promptly
- Continue using supportive measures as needed
- Keep open communication with your healthcare provider
When to Seek Additional Help
Contact your urologist if you experience:
- Worsening erectile function despite treatment
- Sudden changes in sexual function
- New or increasing testicular pain
- Signs of treatment complications
- Significant psychological distress affecting relationships
Living with Varicocele and ED: A Holistic Approach
The psychological and relationship impacts of dealing with both conditions deserve attention alongside medical treatment.
Mental Health Considerations
Erectile dysfunction—regardless of cause—affects self-esteem, masculinity perceptions, and relationship satisfaction. Studies show that men with ED have significantly higher rates of anxiety and depression. Addressing these psychological components is crucial for comprehensive treatment.
Consider:
- Individual therapy with a sex therapist or psychologist
- Couples counseling to maintain relationship intimacy
- Support groups for men dealing with sexual health issues
- Stress management techniques
- Open communication with partners about concerns and treatment progress
Relationship and Intimacy
Varicocele-related ED affects both partners. Maintaining intimacy requires creativity, patience, and communication. Many couples find that focusing on non-penetrative sexual activities, increasing emotional intimacy, and exploring new ways of connecting can actually strengthen their relationship during treatment.
Frequently Asked Questions
Can varicocele cause permanent erectile dysfunction if left untreated?
While varicocele doesn’t always cause permanent ED, delaying treatment may lead to progressive testosterone decline and worsening symptoms. Research shows that earlier intervention generally produces better outcomes. However, even men who have had varicocele for years can experience improvement with treatment. The key is that prolonged, untreated varicocele may cause testicular damage that becomes harder to reverse over time, potentially leading to more persistent ED and fertility issues.
Will varicocele surgery guarantee improved erectile function?
Varicocelectomy improves erectile function in approximately 50-65% of men with both conditions, but outcomes vary based on individual factors including age, varicocele severity, baseline testosterone levels, and the presence of other ED risk factors. Success is most likely in younger men with higher-grade varicoceles who don’t have significant cardiovascular or psychological contributors to their ED. Some men experience dramatic improvement while others see modest benefits, and a minority may not notice significant changes in erectile function despite successful varicocele repair.
How long after varicocele treatment will erectile function improve?
Most men begin noticing improvements within 2-3 months as testosterone levels rise, with peak benefits occurring at 6-12 months post-treatment. The timeline varies because hormonal normalization takes time, and tissue repair is a gradual process. Some men report earlier improvements in libido (within weeks), while erectile quality improvements tend to follow later. Patience is essential—full benefits may not be apparent until one year after treatment. Regular follow-up with your urologist helps track progress and adjust treatment if needed.
Conclusion: Taking Control of Your Sexual Health
The connection between varicocele and erectile dysfunction is real, supported by substantial medical evidence, and importantly—treatable. If you’re experiencing both conditions, you’re not alone, and effective solutions exist.
The key takeaways:
- Varicocele can contribute to ED through testosterone reduction, oxidative stress, and psychological factors
- Proper diagnosis requires evaluating both the varicocele and erectile function
- Treatment options range from conservative management to surgical repair
- Many men experience significant improvement in sexual function after varicocele treatment
- A comprehensive approach addressing physical, hormonal, and psychological factors produces the best outcomes
Don’t let embarrassment or uncertainty prevent you from seeking help. Modern urology offers sophisticated diagnostic tools and effective treatments that can restore both your sexual function and quality of life. Whether through surgical intervention, medical management, supportive measures like specialized varicocele underwear, or a combination of approaches, solutions are available.
Schedule a consultation with a urologist who specializes in male sexual health and varicocele treatment. Bring your questions, be honest about your symptoms, and work together to develop a treatment plan tailored to your specific situation. Your sexual health matters, and addressing these concerns is an important investment in your overall wellbeing and relationship satisfaction.
For more comprehensive information about varicocele diagnosis, symptoms, and treatment options, visit our complete varicocele guide.
Related Articles

Choose Varicocele Support Designed for Cooling, Lift, and Daily Comfort
You’ve seen why regular underwear often falls short. Now view the purpose-built option made to reduce heaviness, improve support, and feel comfortable enough for everyday wear.

